
We recommend taking this quiz that will help you evaluate your knowledge before starting the tutorial.
The Formation of the Cardiac Septa is based on the structures being separated:
1- Septum formation in the Common Atrium
On about day 26, while atrial remodeling is in progress, the roof of the atrium develops a depression along the midline at the site beneath the overlying outflow tract. On day 28, this deepening depression results in a crescent-shaped myocardial wedge, called the septum primum, which extends into the atrium from the cranial-dorsal wall as the primitive atrial chamber expands (fig. 1).
Septum Primum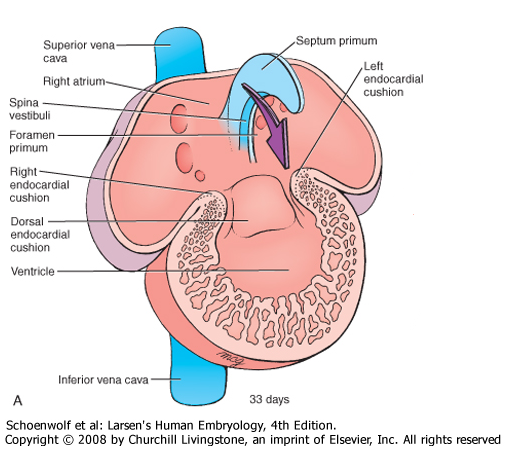 Figure 1
The diminishing foramen between the atria is called the foramen primum (or ostium primum). Before the foramen primum closes, programmed cell death and cell rearrangement in an area near the dorsal edge of the septum primum creates small perforations that coalesce to form a new foramen, the foramen secundum (or ostium secundum). Thus, a new channel for right-to-left shunting opens before the old one closes (fig. 2). |
Septum Secundum Figure 2
While the septum primum is lengthening, a second crescent-shaped ridge of tissue forms on the ceiling of the right atrium, just adjacent and to the right of septum primum. This septum secundum is thick and muscular, in contrast to the thin septum primum (fig. 2). |

Figure 3
The edge of the septum secundum grows, but it halts before it reaches the atrioventricular septum, leaving an opening called the foramen ovale near the floor of the right atrium.
Therefore, throughout the rest of fetal development, blood that shunts from the right atrium to the left atrium passes through two staggered openings: the foramen ovale near the floor of the right atrium, and the foramen secundum near the roof of the left atrium.
This shunt closes at birth because the abrupt dilation of the pulmonary vasculature, combined with the cessation of umbilical flow, reverses the pressure difference between the atria and pushes the flexible septum primum against the more-rigid septum secundum where they fuse and form the interatrial septum.
After the interatrial septum forms, a thinned oval part of the septum remains where the foramen ovale used to be. This thinned, oval area in the interatrail septum is called the fossa ovalis.
Therefore, throughout the rest of fetal development, blood that shunts from the right atrium to the left atrium passes through two staggered openings: the foramen ovale near the floor of the right atrium, and the foramen secundum near the roof of the left atrium.
This shunt closes at birth because the abrupt dilation of the pulmonary vasculature, combined with the cessation of umbilical flow, reverses the pressure difference between the atria and pushes the flexible septum primum against the more-rigid septum secundum where they fuse and form the interatrial septum.
After the interatrial septum forms, a thinned oval part of the septum remains where the foramen ovale used to be. This thinned, oval area in the interatrail septum is called the fossa ovalis.
The video below includes an animation which summarizes the process explained above
Click here to watch the video
2- Septum formation in the Atrioventricular Canal
Lateral view Figure 4
As the septum primum elongates by differential growth, two major endocardial-derived cushion tissues-called the dorsal (or superior) and ventral (or inferior)endocardial cushions-develop around the periphery of the atrioventricular canal. At the end of the 6th week, the dorsal and ventral cushions meet and fuse, forming the atrioventricular septum (or septum intermedium) that divides the common atrioventricular canal into right and left atrioventricular canals. |
Anterior view Figure 5
As the atrioventricular septum forms during the 5th and 6th weeks, the heart is remodeled to align the developing left atrioventricular canal with the left atrium and ventricle, and the right atrioventricular canal with the right atrium and ventricle.
|
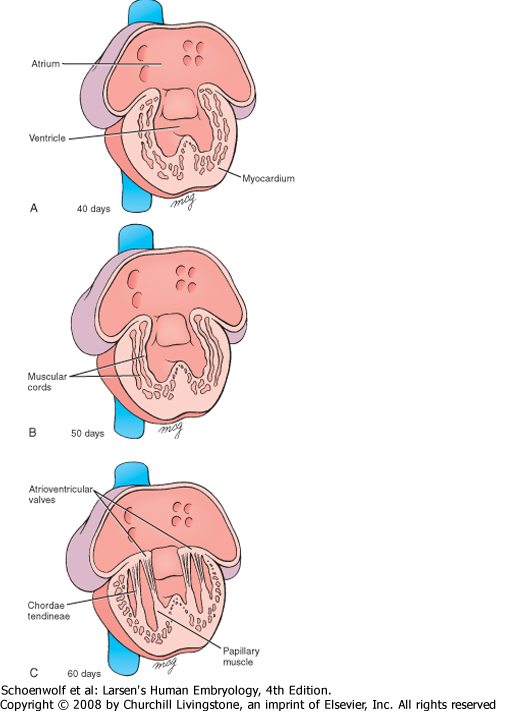
Figure 6
The atrioventricular valves begin to form between the 5th and 8th weeks. These valve leaflets or cusps are firmly rooted in the rim of the right and left atrioventricular canals and are thought to arise from proliferation and differentiation of the adjacent endocardial cushion tissues.
The leaflets are freed from the myocardial wall by remodeling and erosion of the ventricular myocardial wall. This form ventricular outpockets beneath the valvular primordia and leaves thin strands of cells that form the chordae tendineae and small hillocks of myocardium called papillary muscles figure 6.
In this manner, two valve leaflets, constituting the bi-cuspid (or mitral) valve, form in the left atri-oventricular canal, and three, constituting the tricuspid valve, form on the right side.
The video below includes an animation which summarizes the process explained above
3- Septum formation in the Truncus Arteriosus and Conus Cordis (Outflow tract and Ventricles
At the end of fourth week the cardiac outflow tract is divided by the formation of a pair of endocardial-covered conotruncal swellings (ridges) that grow inward along the length of the conotruncal segment.

Figure 7
These swellings eventually fuse to form a septum, the conotruncal septum (sometimes called aorticopulmonary septum), that completely separates the right and left ventricular outflow pathways as shown in figure 7.
The right superior truncus swelling grows distally and to the left, and the left inferior truncus swelling grows distally and to the right. Hence, while growing toward the aortic sac,the swellings twist around each other, foreshad-owing the spiral course of the future septum as shown in figure 7.
After complete fusion, the ridges form the aorticopulmonary septum,dividing the truncus into an aorticand a pulmonary channel.
This spiral arrangement is thought to be driven, in part, by rotational and torsional forces on the outflow tract generated as a consequence of cardiac looping.
When the truncus swellings appear, similar swellings (cushions) develop along the right dorsal and left ventral walls of the conus cordis as shown in figure 8.
The right superior truncus swelling grows distally and to the left, and the left inferior truncus swelling grows distally and to the right. Hence, while growing toward the aortic sac,the swellings twist around each other, foreshad-owing the spiral course of the future septum as shown in figure 7.
After complete fusion, the ridges form the aorticopulmonary septum,dividing the truncus into an aorticand a pulmonary channel.
This spiral arrangement is thought to be driven, in part, by rotational and torsional forces on the outflow tract generated as a consequence of cardiac looping.
When the truncus swellings appear, similar swellings (cushions) develop along the right dorsal and left ventral walls of the conus cordis as shown in figure 8.

Figure 8
The conus swellings grow towards each other and distally to unite with the truncus septum. When the two conus swellings have fused, the septum divides the conus into an anterolateral portion (the outflowtract of the right ventricle) (Fig. 8) and aposteromedial portion (the outflow tract of the left ventricle).
Separation of the right and left ventricles is completed when the muscular interventricular septum fuses with the conotruncal septum and the ventricular side of the atrioventricular septum. Development of this membranous ventricular septum normally occurs between weeks 5 and 8.
Once the conotruncal septum is complete, several modifications also occur in the conus arteriosus. The cushion cells are eventually replaced by a subsequent invasion of the surrounding myocardial cells through the process described earlier as myocardialization.
Here, myocardial cells invade the conotruncus septum and ultimately muscularize this region to form the outflow portion of the definitive right and left ventricles.
Separation of the right and left ventricles is completed when the muscular interventricular septum fuses with the conotruncal septum and the ventricular side of the atrioventricular septum. Development of this membranous ventricular septum normally occurs between weeks 5 and 8.
Once the conotruncal septum is complete, several modifications also occur in the conus arteriosus. The cushion cells are eventually replaced by a subsequent invasion of the surrounding myocardial cells through the process described earlier as myocardialization.
Here, myocardial cells invade the conotruncus septum and ultimately muscularize this region to form the outflow portion of the definitive right and left ventricles.
The video below includes an animation which summarizes the process explained above
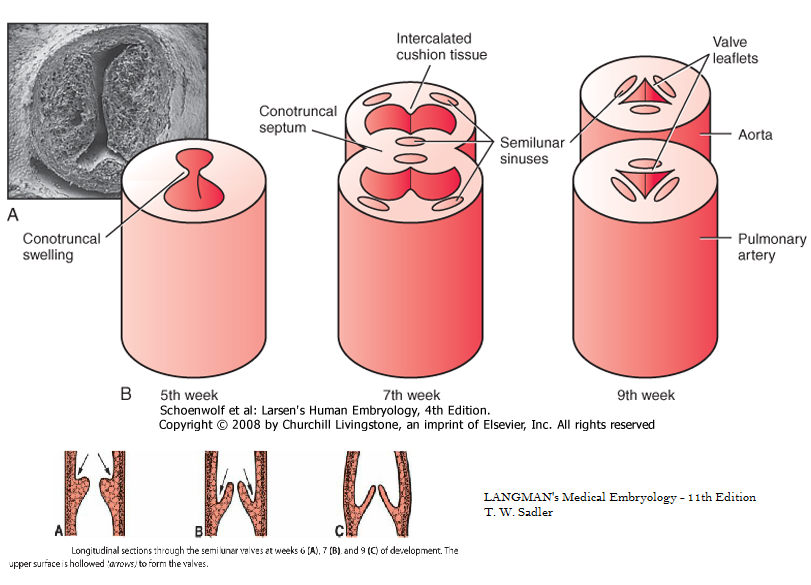
Figure 9
During the formation of the conotruncal septum, two additional smaller cushion tissues form in the opposite quadrants of the outflow tract called the intercalated cushion tissue.
Gradually, the tubercles or cushions hollow out at their upper surface, forming the semilunar valves (Fig. 9).
Gradually, the tubercles or cushions hollow out at their upper surface, forming the semilunar valves (Fig. 9).
Wait what could go wrong: Tetralogy of Fallot, the most frequently occurring abnormality of the conotruncal region (Fig. 10), is due to an unequal division of theconus resulting from anterior displacement of theconotruncal septum.
Displacement of the septum produces four cardiovascular alterations: (a) a narrow right ventricular outflow region,
pulmonary infundibular stenosis: (b) a large defect of the interventricular septum; (c) an overriding aorta that arises directly above the septal defect; and (d) hypertrophy of the right ventricular wall because of higher pressure on the right side.
Tetralogy of Fallot, which is not fatal, occurs in 9.6/10,000 births.
Displacement of the septum produces four cardiovascular alterations: (a) a narrow right ventricular outflow region,
pulmonary infundibular stenosis: (b) a large defect of the interventricular septum; (c) an overriding aorta that arises directly above the septal defect; and (d) hypertrophy of the right ventricular wall because of higher pressure on the right side.
Tetralogy of Fallot, which is not fatal, occurs in 9.6/10,000 births.
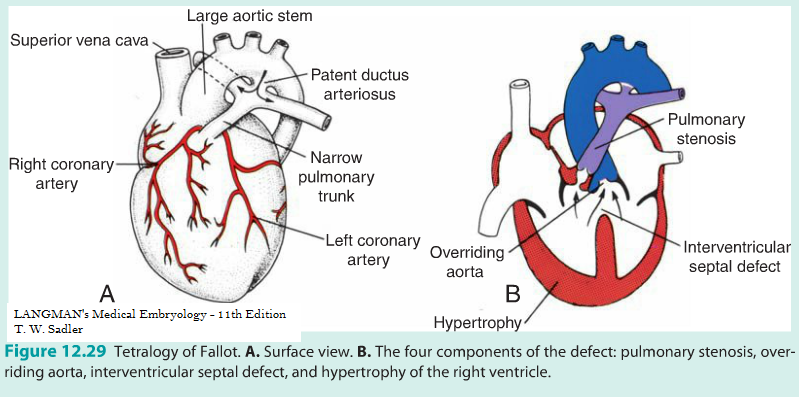
Figure 10
We recommend taking this quiz that will help you evaluate your knowledge after taking the tutorial.
|
Click here to go back to top
|
Prepared by Joy Y. Balta
